
No products in the cart.
Outdoor Adventure
The Not-So-Terrifying Death Stats for 5K Races

04
Oct
Oct
I’m not a huge fan of studies about runners dropping dead—not because the topic is scary or uninteresting to me, but because it’s so hard to calibrate the message properly. When you write a man-bites-dog article, it doesn’t matter how many nuances and caveats you pack in there: some people are inevitably going to walk away with the impression that it’s just a matter of time before some crazy human bites their beagle.
So let me clarify, right off the top, that what follows is mostly a good-news story. In the British Journal of Sports Medicine, a big team of researchers in Britain led by Charles Pedlar of St. Mary’s University published an analysis of every medical encounter at Parkrun events in the United Kingdom between 2014 and 2019. More than two million people participated, racking up 29 million finishes, and 18 of them died. Each of those deaths is extremely sad, but the overall picture is nonetheless encouraging.
The Parkrun phenomenon, if you haven’t encountered it yet, is truly remarkable. Outside columnist Martin Fritz Huber wrote a column about it a couple of years ago (as did I, about my first Parkrun experience). The shtick is fairly simple: every Saturday morning in communities around the world, volunteers host a free, timed 5K run. There are lots of theories, and an emerging body of academic research, seeking to explain why this is different from the ubiquitous community fun runs that already exist. The lack of entry fee helps, as does the fact that it happens every week rather than being a once-a-year event. For whatever reason, as of last year there were seven million people registered in 22 countries, with about 350,000 people participating every week. That’s huge.
With that many people, even very-low-probability events become a matter of when rather than if. In 2014, Parkrun instituted a mandatory system for reporting any medical issues encountered during each event. (The ultimate incentive to get organizers to comply: no finisher results could be posted until it was received.) That’s the database that Pedlar and his colleagues combed through.
There were a total of 84 serious incidents classified as life-threatening, of which 73 involved the heart (48 cases of cardiac arrest, which is when the heart stops; 20 cases of acute coronary syndrome, which includes heart attacks and other blockages of the heart’s blood supply; and five serious arrhythmias). The rest were strokes (eight), respiratory failure (two), and spinal injury (one). There were another 7,492 less serious medical events, most of which involved falls or collisions, and only 698 of which required a trip to the hospital.
So what’s the good news? Of the runners who suffered cardiac arrest, 65 percent survived. That’s way higher than the ten percent who typically survive cardiac arrest when it occurs outside a hospital. The reason: all Parkrun events in the U.K. have to have an automatic defibrillator on hand. One of the potential barriers to further expansion of free events like Parkrun is the question of liability, and whether you need more extensive medical support present. But what makes Parkrun scalable is that it can be put on, week after week, by a small handful of volunteers with a few cones and a smartphone to scan barcodes at the finish line. This analysis suggests that even without medical personnel on the race crew, having a defibrillator is sufficient to dramatically lower the risk of death.
It’s very well established that a single bout of vigorous exercise—like running a 5K, but also like shoveling snow or even having sex—temporarily raises your risk of a heart attack, but regular exercise lowers your risk over the long term. You can see that trade-off in action in the results. Here, for example, is a graph that shows how many previous Parkruns had been completed by people who suffered a serious medical event:
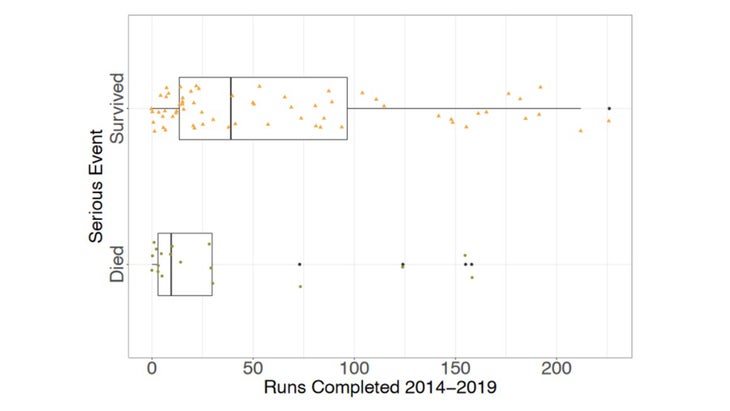
Those who survived (top) tended to have completed far more previous runs than those who didn’t (bottom). Similarly, the fatal cases tended to have slower finishing times, which may indicate less prior training. The vast majority of the serious incidents, both fatal and non-fatal, took place in men (82 percent) who were over 45 years old (83 percent). None of this is surprising, but the authors do suggest that it might be worth considering targeted educational materials, or perhaps even pre-participation online screening, for older, slower, novice runners—an approach that reduced overall medical encounters by 29 percent in the Two Oceans half marathon and ultramarathon in South Africa.
Still, it’s worth keeping the results in context. At the Two Oceans race, online screening and education reduced the rate of life-threatening medical events from 56 per 100,000 runners to 21. For the much shorter Parkruns, held in the temperate weather of Britain, the rate was just 0.3 per 100,000. That’s not too different from the rate of 0.8 sudden cardiac deaths per 100,000 observed in a study of three million marathon finishers back in 2007. The notable detail in that study: hospital admission data showed that for every sudden cardiac death during a marathon, two car-crash deaths were avoided thanks to street closures during the race. That’s the comparison that’s worth remembering. Yes, running is dangerous—but not as dangerous as not running.
For more Sweat Science, join me on Twitter and Facebook, sign up for the email newsletter, and check out my book Endure: Mind, Body, and the Curiously Elastic Limits of Human Performance.